
AUSTERE CARE: NETCCN is meant to provide military medical care to the austere environments likely to be found during multidomain operations, like the ones these U.S. Marines found in August 2019 during an exercise in Kuwait. (Photo by Cpl. Miguel A. Rosales, 1st Marine Division)
NETCCN promises to bring high-quality care to patients, digitally.
by Ramin A. Khalili
If you know Matthew Quinn, the new science director at the U.S. Army Medical Research and Development Command’s (USAMRDC) Telemedicine and Advanced Technology Research Center (TATRC), then you know that technology—emerging concepts, practical uses and all of its endless possibilities—is in his blood. A former Army officer and engineer turned Silicon Valley executive, Quinn has, in many ways, spent his entire professional life looking for the so-called “next big thing” in technology. Now, upon his return to federal service, he may have just found it.
“This is a really powerful project,” said Quinn of TATRC’s newest brainchild, the National Emergency Telecritical Care Network (NETCCN)—the premise of which originated in part with Col. Jeremy Pamplin, the center’s director and a critical care physician. “There is an immediate need for these kinds of capabilities.”
In simple terms, NETCCN sits at the intersection of the kind of military medical care required to support the austere environments likely to be found during multidomain operations and the rapid growth of digital health technologies and telehealth opportunities that are becoming pervasive in the civilian world. In essence, by applying the vast technical and clinical knowledge found in both realms, the center hopes to build NETCCN into a new digital health system that will revolutionize overall care for patients during disasters and, possibly, more broadly as well. In more detailed terms, NETCCN is a cloud-based, low-resource, stand-alone health information management system with the capability of creating innumerable “virtual critical care wards” to bring high-quality care capability—via current handheld mobile devices—to nearly every bedside in the country.
It is, in many ways, a substantial undertaking.
“It’s not just a technology thing,” said Quinn, the former tech-sector executive now coordinating NETCCN’s development from his home office during the pandemic. “This is clinicians working with technologists on a brand new care model.”
That Quinn would be working from home (like many of his colleagues, of course) during the coronavirus outbreak is somewhat ironic given the catalyst for NETCCN is the novel coronavirus itself. Disasters of any kind notably stress health care infrastructure and staff, as there are simply not enough qualified clinicians to provide care during large-scale emergencies. And while many health systems across the country already have existing digital models of care for smaller, more localized emergencies (think telehealth consultations for victims of car crashes or stroke), the team at TATRC initiated the NETCCN effort by asking those same health systems, along with clinicians affiliated with the Society of Critical Care Medicine (SCCM), how they would refine those models for the current pandemic.
That’s when TATRC knew they were onto something.
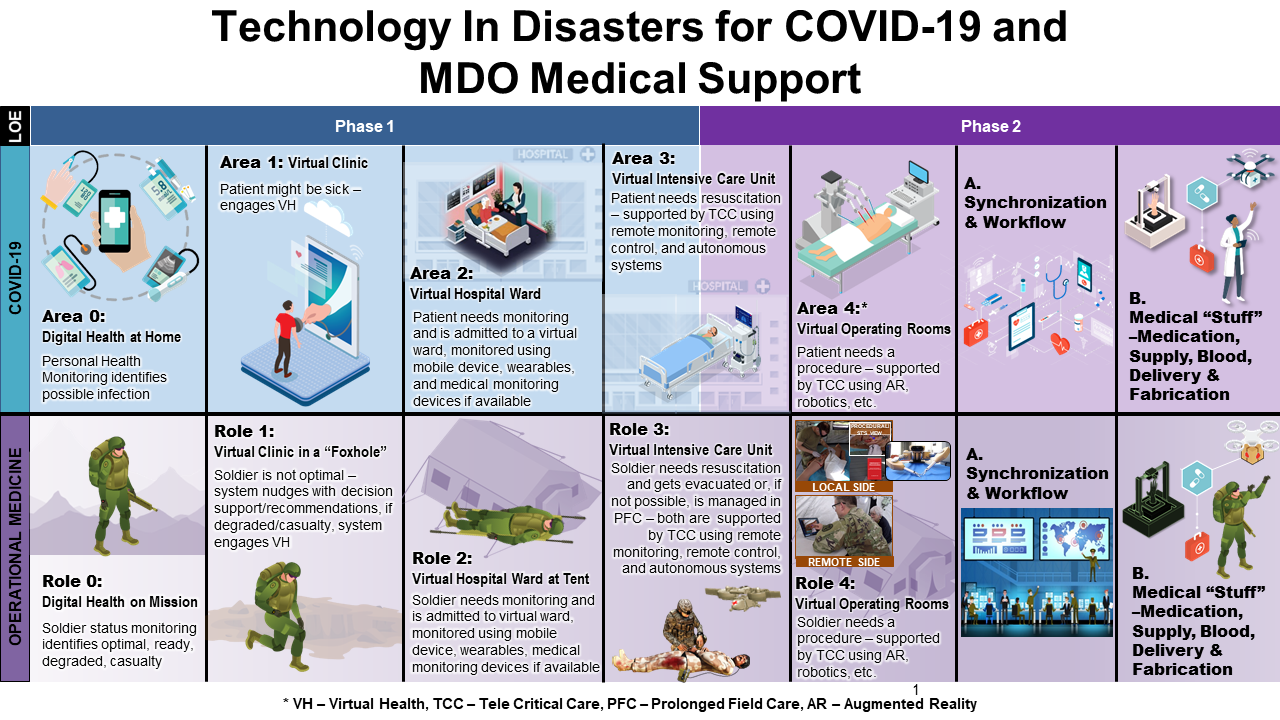
OH, THE POSSIBILITIES: There are many potential uses and applications for NETCCN in the military operational and civilian worlds, but the system will require more work before implementation. (Graphic courtesy of TATRC)
ALWAYS ON CALL
“You can get extra beds and you can maybe get extra ventilators,” said Quinn, “but what you just can’t surge quickly enough is the expertise required to manage these complex patients.” In other words, you can’t just order new nurses or cardiologists from a catalog. But what if you could access them online when needed?
According to Quinn, many of those aforementioned health systems told TATRC they were already in the process of refining their own digital models to be deployed quickly and to work as much as possible in both bandwidth-constrained areas and with current mobile devices. He’s quick to point out that rural America has been dealing with these kinds of supply-and-demand issues for years; problems solved in large part thanks to these same kinds of digital telehealth solutions. What sets NETCCN apart from standard telehealth care, then, is that it will operate from point-to-point (“from anywhere to anywhere,” in Pamplin’s words) as opposed to the traditional “hub-and-spoke” model, which is dependent on a single outlet (like a hospital or university) broadcasting instruction to a series of single users.
“We anticipate that there’s going to be a need for doing this community-wide, and then even statewide and regionally and nationally,” said Quinn, noting a few recent pandemic-inspired examples. “For example, when the rest of the country needed New York’s help or the Northeast’s help, how could we have facilitated that [with NETCCN]? And then how could we have facilitated the parts of the country that weren’t afflicted [at the time] when they needed it?” The idea is to surge medical specialists when needed, with no travel required.

LONG-DISTANCE SUPPORT: NETCCN is being developed with the goal of dramatically improving care for warfighters in austere environments, like these deployed Soldiers who participated in a mass casualty exercise in September 2019 at Al Asad Airbase, Iraq. (Photo by Sgt. 1st Class Tracy L. Korff, 641st Regional Support Group)
GAINING TRACTION
But just as with any great idea in the military medical world, the acquisition process is the critical driver of success. For the NETCCN project, that’s where Jeanette Little comes in.
“My job is to make it happen,” said Little, a lab leader at TATRC whose office is located at Fort Gordon in Augusta, Georgia—the home of Army Cyber Command. “We do all the rubber-meets-the-road stuff.”
That proverbial road, however, was always designed to be a short one. Adhering to an incredibly accelerated timeline, TATRC sent out a request for proposals for NETCCN in mid-April, with hopes of having the entire network up and running by late October. A process that started with 600 participants on the initial proposer’s call ultimately led to 79 proposals. “We were hoping to get maybe 30,” said Little. Currently, the center is winnowing down that group from nine teams to six teams; ultimately planning to settle on three final teams that will then be asked to develop the network in a collaborative fashion. “I’ve never seen so much scientific rigor put into an acquisitions process,” she said.
Indeed, part of the reason such a fast-moving effort is possible can be attributed to the center’s reliance on the USAMRDC partnership with the Medical Technology Enterprise Consortium (MTEC). A nonprofit corporation comprised of hundreds of private, academic and not-for-profit organizations, MTEC is designed to accelerate the translation of medical technologies into solutions focusing chiefly on the health of U.S. military personnel and veterans. An integral part of MTEC’s partnership with DOD—and the key mechanism allowing NETCCN to progress as quickly as it has—rests within its use of the other-transaction authority (OTA), a powerful tool that allows MTEC to operate a solicitation process in a more transparent and collaborative manner, tearing down traditional acquisition barriers restricting government-industry interactions.) It is perhaps the MTEC brand name that helped bring such headliners as Microsoft, T-Mobile, Emory Healthcare and the University of Pittsburgh (among others) to the table as part of various teaming arrangements for NETCCN. “We are very deliberate because we need a working solution to help with all kinds of health-related issues, not the least of which is the current pandemic,” said Little.
“This isn’t a science experiment,” Quin added. “It’s not building stuff from scratch. In a matter of 60 to 90 days, we’re going to be out there with these tools.”
Beyond the pandemic—and outside of other practical applications on the home front such as large-scale disaster situations—there can be no doubt the NETCCN would clearly translate well to the future battlefield; providing increased Soldier care in austere environments; and particularly with regard to the current posture of DOD as it relates to multidomain operations. Indeed, the NETCCN team is currently working on a slew of models designed to project how, exactly, the network would be used in dense urban environments and on ships. Given the network’s “anywhere to anywhere” capabilities, the capacity to empower, for instance, medics to work far beyond the scope of their license on complicated care issues with support from literally any echelon of care would be a game-changer for force health and resilience.

COVER YOUR BUDDY: NETCCN was originally developed to help aid care for COVID-19 patients nationwide, with an eye toward helping both the warfighter and the larger civilian population during disaster relief efforts in the future. Here, Navy Lt. Tiffany Bradley participates in fit testing for an N95 respirator and survival mask at Naval Hospital Okinawa, Japan, on March 27. (Photo by 1st Lt. Tori Sharpe, U.S. Marine Corps)
For right now, however, more work needs to be done. Data collection (as in the analysis of data culled from the testing of prototype NETCCN platforms and then enabling contribution of data to a “data commons” repository) remains a challenge in such a fast-paced project (such efforts would be “showstoppers” in any other arena at any other time, admits Quinn), and yet that hasn’t stopped the NETCCN’s progress in the least. In fact, TATRC officials have already set their sights on using said data for developing future analytical models and possibly for artificial intelligence purposes.
“There’s value in what we’re doing,” said Quinn. “Not only for the current crisis, but for future emergencies as well.”
For more information about TATRC, go to https://www.tatrc.org/www/about/. For more information about the USAMRDC, go to https://mrdc.amedd.army.mil/.
RAMIN KHALILI is a writer with the USAMRDC Public Affairs Office. Before assuming his current role, he spent five years as the knowledge manager for the USAMRDC’s Combat Casualty Care Research Program. During his previous work as a broadcast journalist, he earned an Associated Press Award for his work in Phoenix, Arizona, before serving as chief NASA correspondent for CBS in Orlando, Florida. He holds a B.A. in communications from Penn State University.
Read the full article in the Fall 2020 issue of Army AL&T magazine.
Subscribe to Army AL&T News – the premier online news source for the Army Acquisition Workforce.  Subscribe
Subscribe